
Snapshots of Maternity Care in Rural New Hampshire:
A Photovoice Project
The project team
Sanam Roder-DeWan, Principal Investigator
Kailene Jones, Community Research & Engagement Manager
Riley Carbone, Research Assistant
Nicole Roeper, Research Assistant
Cheri Bryer, Facilitator
Daisy Goodman, Co- Investigator
Julie Bosak, Co-Investigator
Participant-Researchers
We recruited 17 participant-researchers, five of whom were pregnant. Five key themes emerged from the work. Participants make decisions about maternity care by balancing quality and access, feel unheard and actively advocate for their preferred maternity care, experience isolation especially in the postpartum period, and experience fear and stress due to access challenges that force them to make compromises and find creative solutions.

Brandi Ash
Mother of 1.
Lisbon, NH

Lisa Coloumbe
Mother of 1.
Berlin, NH

Suzanna Crowner
Mother of 2 rainbow babies & 2 angel babies.
Concord, VT

Katy-Lynn Dubay
Mother of 4.
Berlin, NH

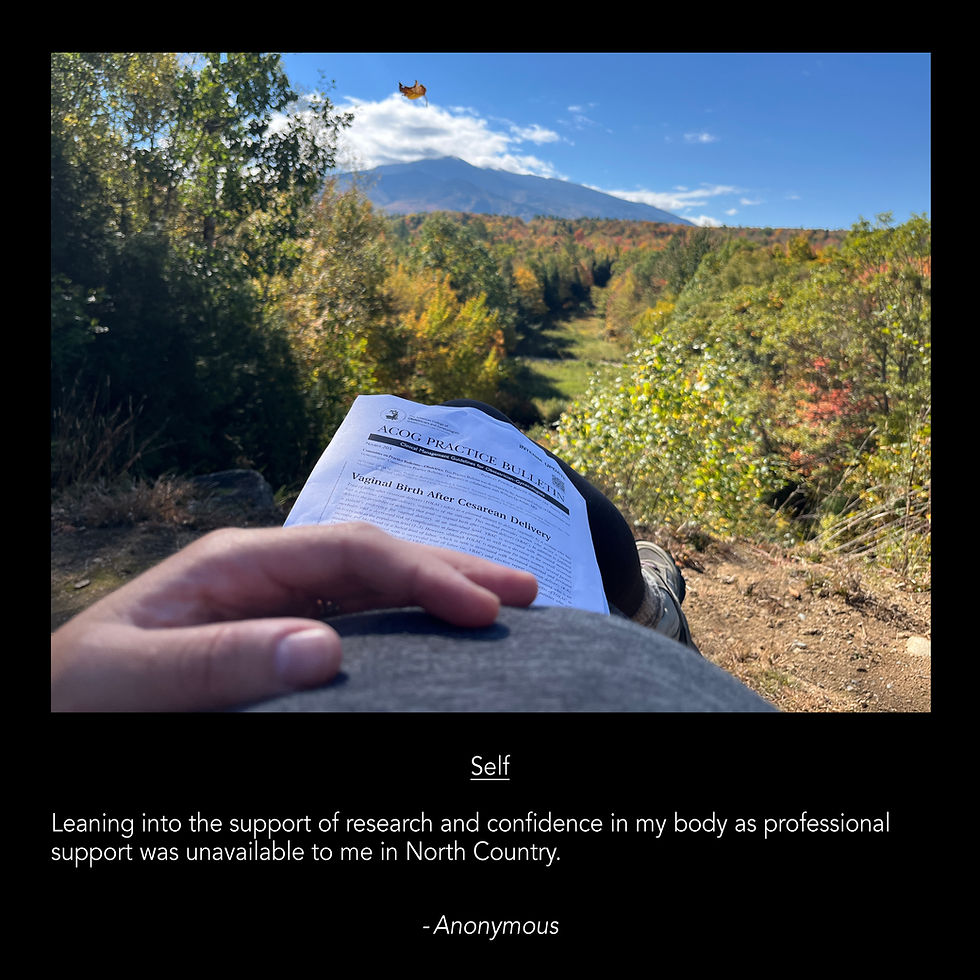
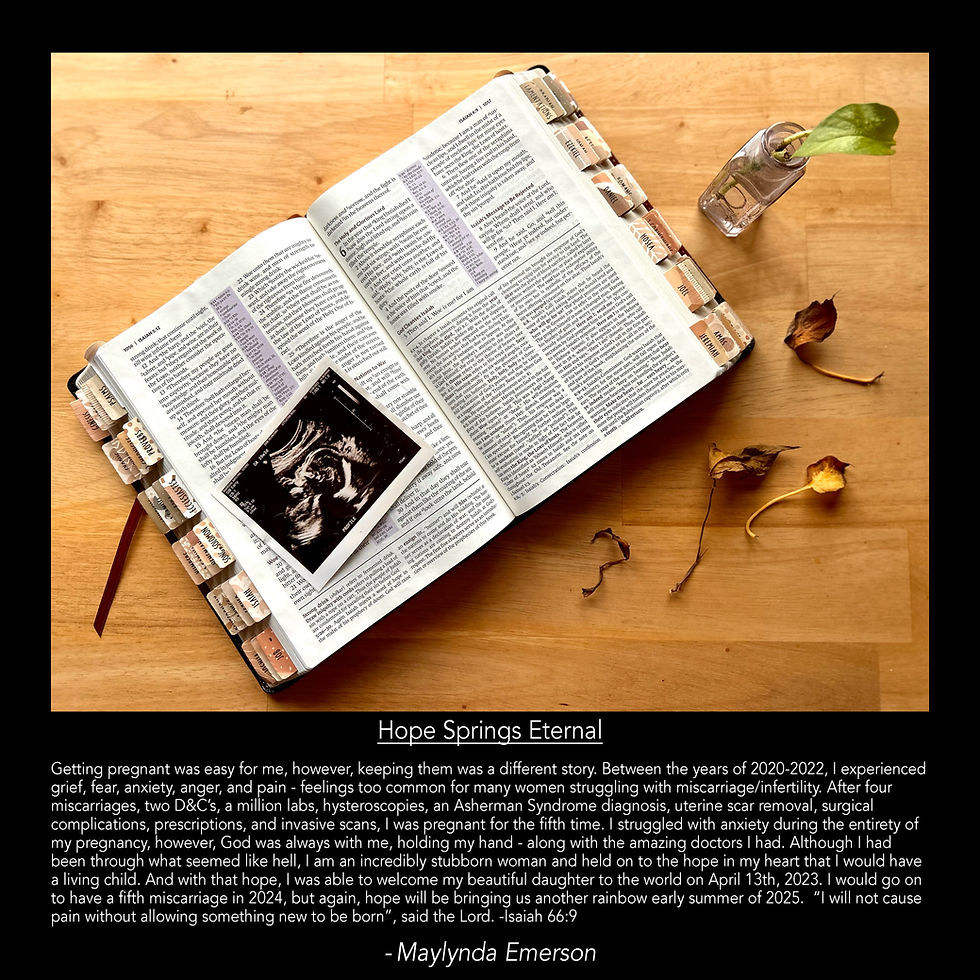
Maylynda Emerson
Mother of 2 rainbow babies & 5 angel babies.
Stark, NH

Jaimie Hawkins
Mother of 4
Berlin, NH

Jessie Ingerson
Mother of 1 rainbow baby, 1 angel baby, & 2 bonus boys
Jefferson, NH

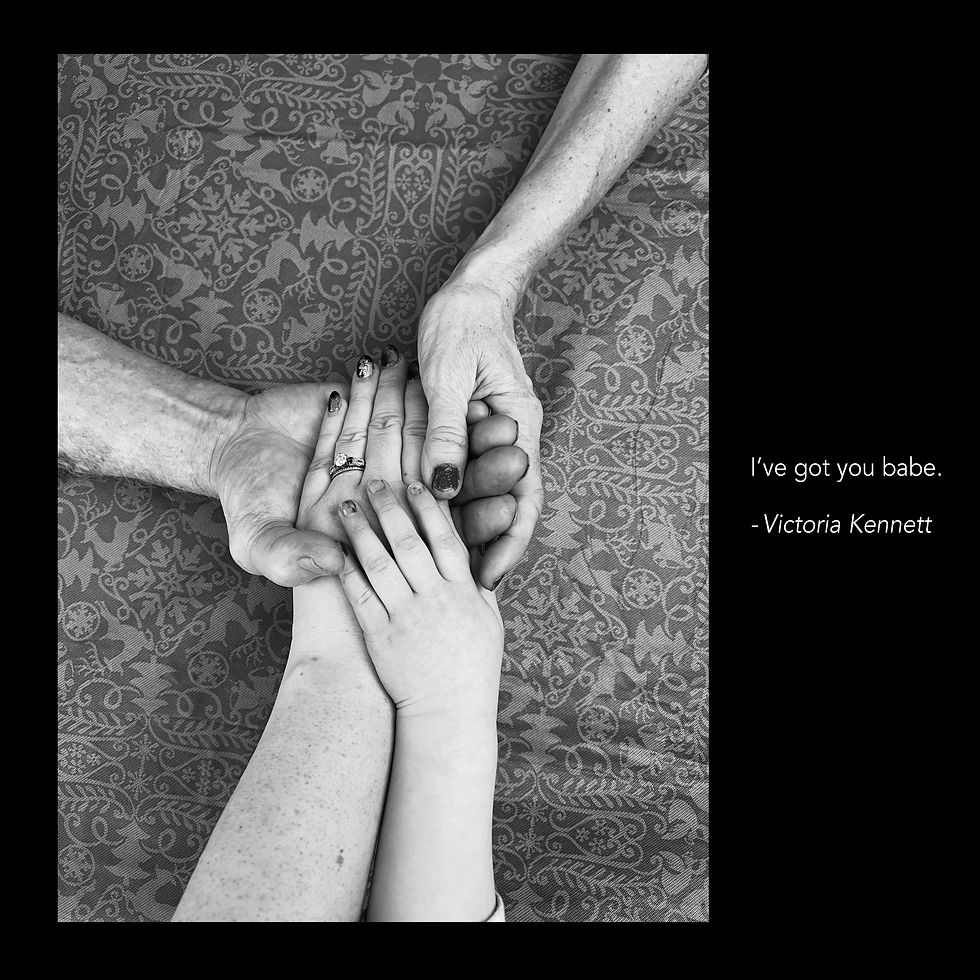
Victoria Kennet
Mother of 2
Colebrook, NH

Katherine Kenyi
Mother of 5
Dalton, NH

Brianna Lareau
Mother of 4.
Piermont, NH

Casandra Mercer
Mother of 5
Berlin, NH

Ashley Shaw
Mother of 2
Berlin, NH

Tiffany Sweatt
Mother of 2.
Errol, NH

Rose Toner
Mother of 5
Littleton, NH

2 Anonymous
Mother of 3
Mother of 4

Brittany Leighton
Mother of 3.
Groveton, NH
FIVE KEY THEMES





Make compromises and find creative solutions to balance maternity care quality & access







Experience a mismatch between needs and services available





Feel unheard and actively advocate for their preferred maternity care




Experience isolation especially in the postpartum period and during pregnancy loss






Are thriving in motherhood and building resilience even in the face of challenges






Access to maternity care in New Hampshire has decreased over the last 20 years due to obstetric unit closings; 11 of 26 birthing units have shuttered services.
Background: Access to maternity care in New Hampshire has decreased over the last 20 years due to obstetric unit closings; 11 of 26 birthing units have shuttered services. Closings have disproportionately occurred in impoverished rural communities. Current literature does not describe the impact on rural families or offer people-centered mitigating strategies. This study describes the experiences of rural people impacted by closings and explores potential solutions.
Methods: We used Photovoice, a qualitative participatory action research method in which participants represent their lived experiences through photography, to achieve study objectives. We partnered with a community organization to recruit pregnant and parenting people from the North Country of New Hampshire (participant-researchers) who attended a series of three workshops. In the first workshop cohorts learned photography skills and prepared to take photos in their communities using prompts about maternity experiences, challenges, and supports. In workshop two participants used their photos to share birth stories, identified common themes, and developed unique prompts for the next assignment. In workshop three they again presented photos and identified themes, then discussed using the photos for advocacy and explored interventions. All three cohorts gathered for a fourth session where participatory thematic analysis of photos and captions was conducted by participants and study team members.. Study team members used photo-elicitation during workshops to deepen stories. Photos, captions, and workshop dialogue were coded and analyzed using a phenomenological interpretive approach.
Results: We recruited 17 participant-researchers, five of whom were pregnant. Four key themes emerged from the work. Participants make decisions about maternity care by balancing quality and access, feel unheard and actively advocate for their preferred maternity care, experience isolation especially in the postpartum period, and experience fear and stress due to access challenges that force them to make compromises and find creative solutions.
Conclusions: Poor access to maternity care shifts the burden of ensuring a positive healthcare experience from the health system to rural families. Solutions must be tailored to the realities of poor access and isolation.